
Families in Massachusetts are hearing more about “intentional communities” as a new housing option for individuals with intellectual and developmental disabilities. These models are often presented as innovative, community‑based solutions. For some individuals, they can be a good fit.
But intentional communities are not the same as Intermediate Care Facilities for Individuals with Intellectual Disabilities (ICF/IID). The growing demand for congregate care and intentional communities is coming from families of individuals with significant needs. Corporate HCBS providers and their trade associations, which historically opposed intentional communities, are now signaling support, largely because they want to control any future congregate‑care development and the funding that comes with it. It is important for families and policymakers to recognize the difference between these two congregate care models.
What Is an Intermediate Care Facility(ICF/IID)?
I explain here:
Understanding the distinction is essential for families, policymakers, and advocates who are trying to navigate a system that already struggles to meet the needs of individuals with high medical and behavioral complexity.
⭐ What Are Intentional Communities?
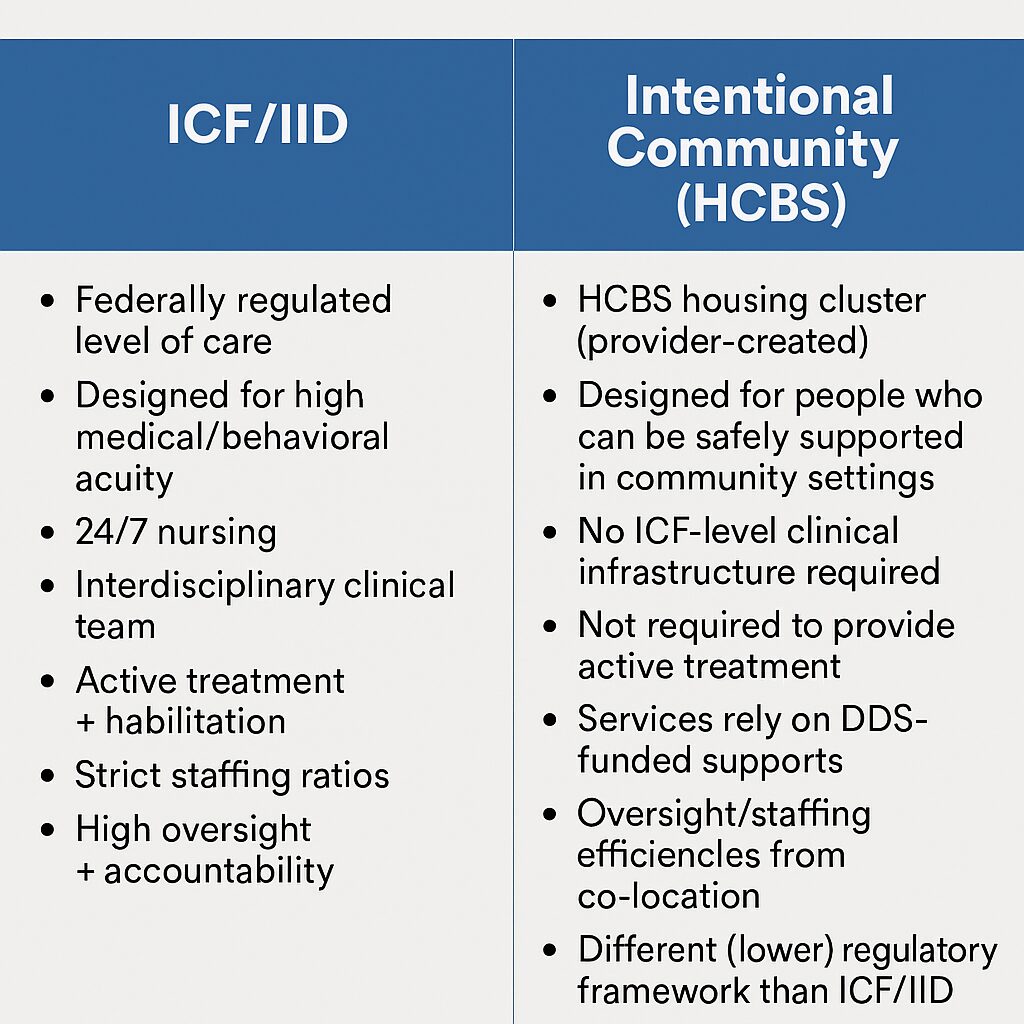
Intentional communities are essentially HCBS‑based housing clusters created by private providers. They centralize the location of homes, which can make internal oversight and staffing more efficient. But it’s important to note that they are still Home and Community‑Based Services (HCBS) programs — not ICF/IID programs — and therefore operate under a completely different regulatory framework.
Because they are HCBS, intentional communities:
- do not provide the level of clinical oversight required in an ICF/IID
- are not required to deliver active treatment
- rely on DDS‑funded services rather than a federally regulated model
- are designed for individuals who can be safely supported in a community‑based setting
In other words, intentional communities may offer a sense of community and shared resources, but they do not provide the clinical infrastructure that some individuals require.
⭐ What Makes ICF/IID Different?
ICF/IID programs are a federally regulated level of care designed specifically for individuals with significant medical, behavioral, or developmental needs. They must provide:
- 24/7 nursing
- interdisciplinary clinical teams
- active treatment
- habilitation services
- strict staffing ratios
- federal oversight and accountability
ICF/IID is not simply “more staff” or “more structure.” It is a clinical model, not a housing model.
For individuals with high acuity needs, this distinction is not academic; it is the difference between being safely supported and being placed in a setting that cannot meet their needs.
⭐ Why the Distinction Matters in Massachusetts
There has been a noticeable push in Massachusetts to use intentional communities as a way to expand housing options, especially for individuals with higher needs. While these communities may help address some capacity issues, they remain a lower level of care than ICF/IID and are not intended to replace the clinical infrastructure that some individuals require.
When intentional communities are presented as an alternative to ICF/IID, families may mistakenly believe they offer equivalent supports. They do not.
Massachusetts needs both:
- community‑based HCBS options for those who can be safely supported there
- and
- ICF/IID programs for individuals whose needs exceed what HCBS can provide
Replacing one with the other leaves the highest‑need individuals without appropriate care.
⭐ Bottom Line
Intentional communities can be a valuable addition to the HCBS landscape, but they are not a substitute for ICF/IID. They operate under different rules and offer different levels of support.
For families navigating the system and for policymakers shaping it, clarity on this distinction is essential. Real choice requires accurate information and a full continuum of care, not the rebranding of lower‑acuity models as solutions for high‑acuity needs.