
MA IDD Lawsuit Series: Part 1

Massachusetts often describes itself as a national leader in community living for people with intellectual and developmental disabilities (IDD). But the historical record shows something very different: the state expanded community services only when forced by federal courts, and only after years of failing to meet basic legal obligations.
No case exposes this gap between rhetoric and reality more clearly than Rolland v. Cellucci, a class‑action lawsuit on behalf of nearly 2,000 people with IDD living in nursing homes.
Preadmission Screening and Resident Review (PASRR
Under the Nursing Home Reform Act (OBRA ’87), states must identify people with IDD entering or living in nursing homes, evaluate their needs, and provide specialized services — including:
Active Treatment, Skill Building Supports, Therapies, and Opportunities for Community Living
Massachusetts wasn’t doing any of this.
Residents with IDD were placed in nursing homes because it was cheaper for the Department of Developmental Services and administratively easier, even though nursing homes were never designed to provide the services federal law required.
Why So Many People Ended Up in Nursing Homes
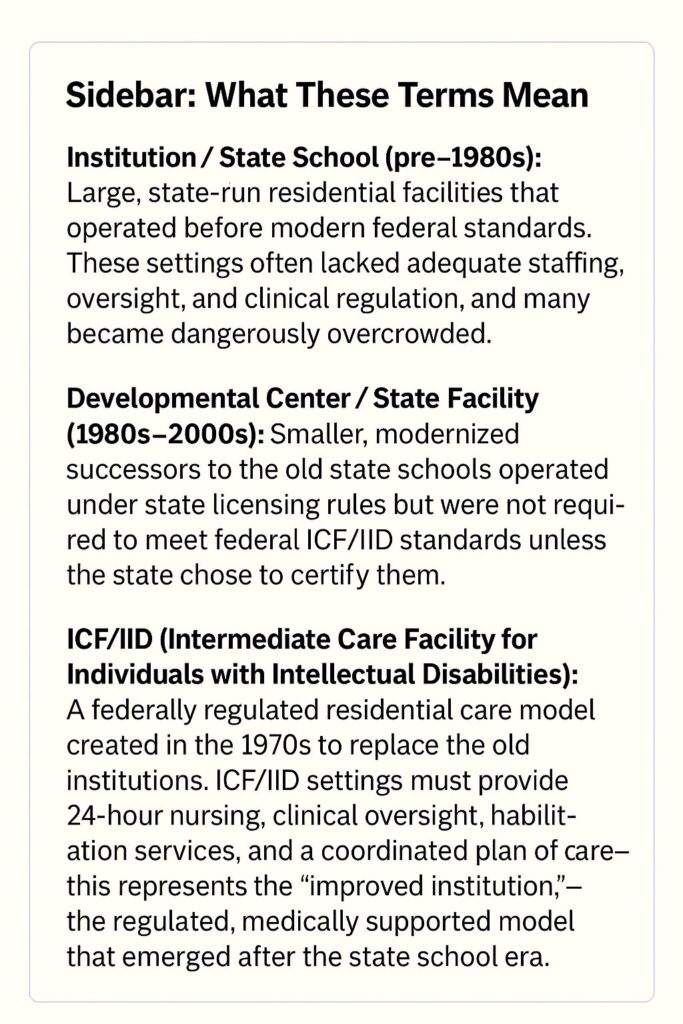
A critical piece of context is how so many people with IDD ended up in nursing homes to begin with. In the aftermath of the Ricci lawsuit, Massachusetts was under pressure to show that it was reducing the population of its state‑operated intermediate care facilities (ICF/IID). Rather than invest in high‑acuity community options or maintain appropriate ICF/IID placements, the state took an easier path: it quietly moved people into nursing homes. These transfers were counted as “community placements,” even though nursing homes provided no active treatment, no habilitation, and no meaningful integration — and were, in fact, a more restrictive setting than the ICF/IID facilities people had been moved out of.
Why Families Couldn’t Stop These Placements
Many residents had guardians, but guardianship didn’t stop these moves. Families were told the transfer was necessary or unavoidable, and many people had no guardian left to speak for them. Others had state‑appointed guardians with no practical ability to object. In the end, people were moved into a more restrictive setting with no meaningful way to refuse.
Most disability organizations at the time supported the state’s push to reduce the census of the large state‑run ICF/IIDs. Groups like Arc of Massachusetts and other “community‑only” advocates viewed any move out of an intermediate care facility (ICF/IID) as progress and did not oppose the transfers into nursing homes.* Families who tried to resist these placements often found themselves with little organizational support. The Coalition of Families and Advocates (COFAR) was one of the few organizations that objected, warning that people with high‑acuity needs were being moved into settings that were even more restrictive and lacked the services federal law required.
What the Rolland Lawsuit Found
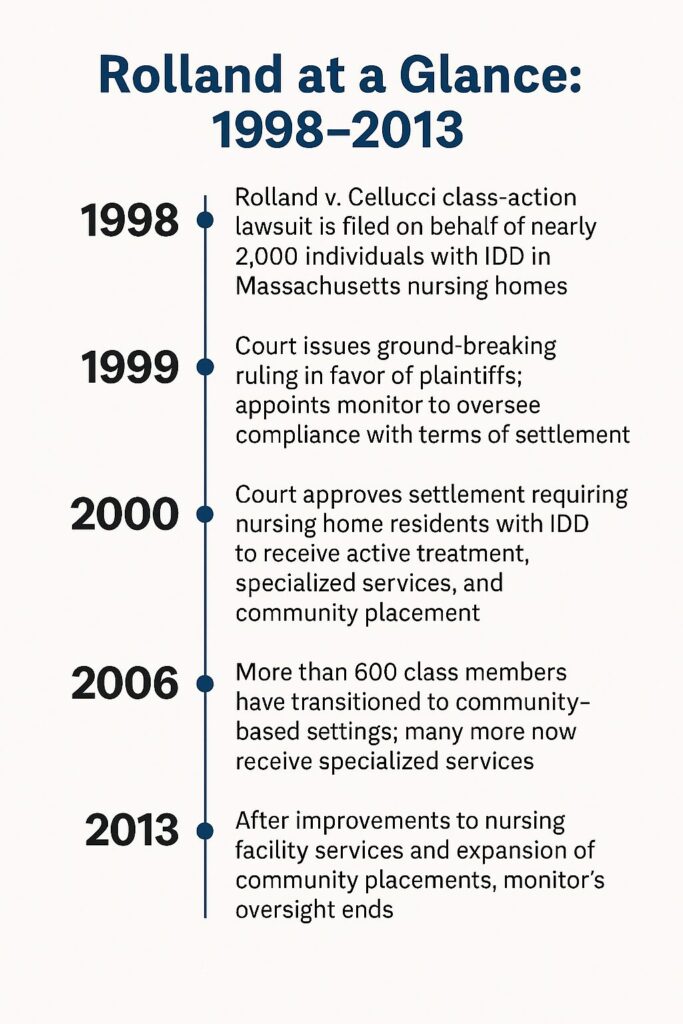
Filed in 1998, Rolland argued that Massachusetts had:
- Failed to screen residents with IDD
- Failed to provide specialized services and active treatment
- Failed to divert people from unnecessary institutionalization
- Failed to offer community placement when appropriate
The state entered a settlement in 1999 requiring community placement for 1,100 people and active treatment for all class members.
But it still didn’t comply.
Over the next decade, the court issued repeated findings of noncompliance, appointed a monitor, and imposed federal active‑treatment standards. A second settlement in 2007 required another 650 community placements. The case wasn’t dismissed until 2013 — after 14 years of oversight.
A Critical, Overlooked Fact
Not everyone stayed in the community.
Some individuals moved out of nursing homes under Rolland later returned to state‑operated intermediate care facilities (ICF/IID) because:
- Their needs were too complex
- Community placements broke down
- Safety and health concerns emerged
Even in a lawsuit designed to promote community living, the state ultimately relied on ICF/IIDs for people with the highest needs. This directly contradicts today’s claim that “everyone can be served in the community.”
What Rolland Actually Shows
1. Massachusetts did not expand community living voluntarily
It took a federal lawsuit, a court monitor, and years of judicial pressure before the state acted.
2. The state repeatedly failed to meet federal requirements
Even after agreeing to the settlement, Massachusetts continued to deny active treatment, specialized services, and diversion planning.
3. Community placement happened only under court order
More than 1,700 people moved to the community — but only because the court required it.
4. ICF/IIDs remained essential
The state relied on them when community placements failed, proving that a full continuum of care is necessary.
5. Rolland addressed only one part of the system
It focused on nursing homes. It did not fix Home and Community-Based Services (HCBS) quality, staffing shortages, or the absence of active treatment in community settings.
What Remains Today
When Rolland ended in 2013, all court oversight ended with it. The settlement obligations do not continue without enforcement.
Federal law still requires active treatment and proper PASRR evaluations — but only if someone files a complaint. There is no automatic auditing, no monitor, and no independent watchdog
Massachusetts is effectively operating on the honor system, and history shows the state complies only when compelled by litigation.
Families of individuals with IDD — whether aging or medically complex — now face the same uncertainty that existed before Rolland
Will My Loved One End Up in a Nursing Home with No Meaningful Activities?
Legally, the state cannot return to the pre‑Rolland pattern of warehousing people with IDD in nursing homes without specialized services. But the financial incentives remain:
- DDS can avoid costs to their own budget by shifting high‑acuity individuals into MassHealth‑funded settings
- Nursing homes appear cheaper for DDS than providing intensive supports in the community or in ICF/IID care.
Without renewed legal action or federal oversight, nothing prevents the state from quietly relying on nursing homes again.
Rolland was a warning, not a guarantee.
When “Community Living” Depends on Families, Not the State

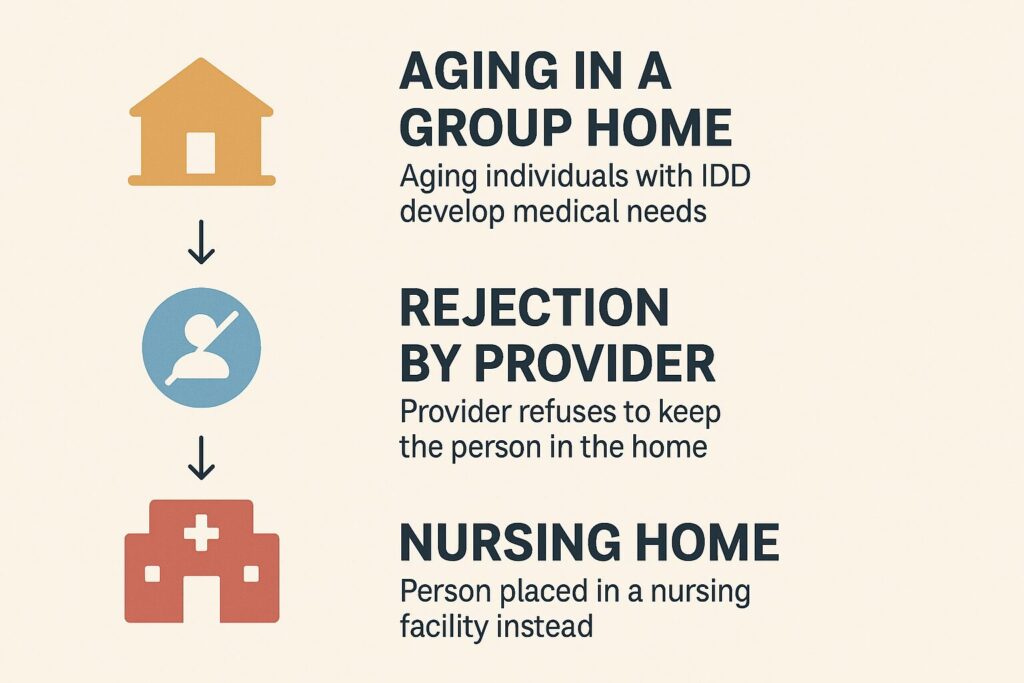
Many individuals in self‑directed services and shared living and even in group homes are stable because their families are filling the gaps — coordinating care, managing crises, providing medical oversight, and doing the day‑to‑day work. These arrangements function because families are alive and able to carry the load.
The state has no plan for what happens when those families are gone.
There is no automatic transition to high‑acuity supports, no guaranteed staffing, no crisis‑prevention infrastructure, and no pathway to ICF/IID care. When a medically complex individual loses their family support, the system can default to the only setting that can accept someone: a nursing home.
Why Every Special Needs Family Should Care About Preserving ICF/IID Care — Even If Community Living Works Today
Many parents feel confident that community living is the only path for their adult children with IDD — and for some individuals, it works beautifully. But community living is not a lifetime guarantee. Needs change. Health changes. Behavior changes. Support systems collapse. Providers withdraw. Funding priorities shift. And families age.
At some point in a person’s life, additional care will be needed — sometimes suddenly, sometimes gradually, but inevitably for many individuals with IDD.
And here is the truth families are rarely told:
ICF/IID care is the only setting specifically designed for people with intellectual and developmental disabilities who need 24/7 clinical, behavioral, and habilitative support. Nursing homes are not.
If the remaining ICF/IID facilities at Wrentham and Hogan are shut down, the state will have only one place to send medically complex or behaviorally complex individuals when community supports fail: a nursing home.
Not because it’s appropriate.
Not because it’s safe.
But because it’s the only option left.
This is not a hypothetical risk.
It is exactly what happened before Rolland — and it is exactly what will happen again if the state eliminates the last ICF/IID facilities.
Families who believe “my child will always live in the community” need to understand:
Community living works only as long as the person’s needs stay within what the community system can handle. When needs exceed that capacity, the system must have a high‑acuity option — or it defaults to nursing homes.
Preserving ICF/IID care is not about rejecting community living.
It’s about protecting your child’s future when community living is no longer enough.
What Comes Next
To understand why Rolland unfolded the way it did, we have to go back to the lawsuit that reshaped Massachusetts long before Rolland was filed: Ricci v. Okin — a case that promised transformation but left a complicated legacy.
Ricci transformed Massachusetts for the better. It improved institutions, created the foundation for community services, and established standards the state had never met before. But in the years that followed, the state and influential advocacy groups rewrote the meaning of Ricci, using its success to justify decisions that Ricci never intended — including the quiet transfer of medically complex people into nursing homes. That story comes next in our MA IDD Lawsuit Series.
If you missed the introduction to our five-part series, you may read it here.
Learn more about intermediate care facilities (ICF/IID) here.
Join Us Today
We are building a coalition to protect choice, dignity, and high‑acuity care for individuals with IDD. Your voice matters.
Join the Saving Wrentham and Hogan Alliance
Join the Saving Wrentham and Hogan Facebook Group
*This description of advocacy positions during the ICF/IID census‑reduction period is supported by contemporaneous public testimony from The Arc of Massachusetts, DDS policy documents from the 1980s–2000s outlining stakeholder support for institutional closure, the Rolland v. Romney litigation record documenting the state’s use of nursing homes for individuals with developmental disabilities, and COFAR’s published statements and legislative testimony opposing these transfers.