
MA IDD Lawsuit Series:
Part 4
Hutchinson v. Patrick revealed a simple but devastating truth: when Massachusetts lacks the services people need, it turns to nursing homes—whether the person has an acquired brain injury or an intellectual disability. This case exposed a systemic failure: a state that embraced the language of inclusion while maintaining a service system that excluded people in practice.
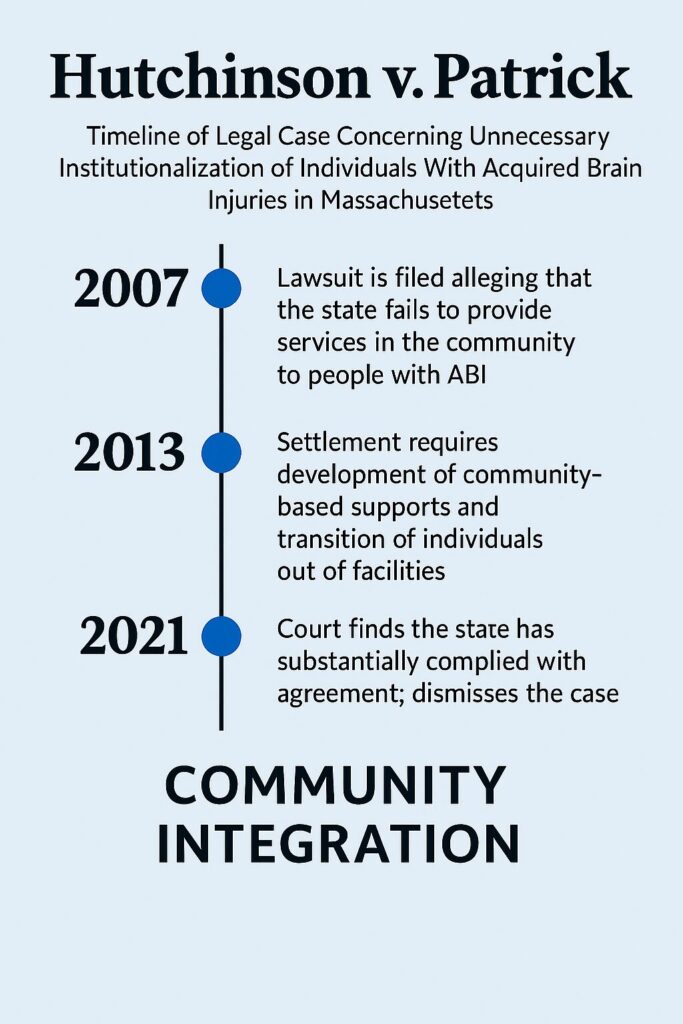
Most people assume that once Massachusetts closed its large institutions and expanded community services, the state finally fulfilled its promise of supporting people with disabilities in integrated settings. But the Hutchinson lawsuit, filed in 2007, exposed a different reality.
Adults with acquired brain injuries (ABI)—medically stable and ready for community living—remained in nursing homes for years because the Commonwealth had never built the services they needed. The pattern echoed Rolland: when Massachusetts lacks appropriate community supports, it turns to nursing homes, whether the person has an acquired brain injury or an intellectual disability. Hutchinson matters for intellectual disability advocates because it showed the failure wasn’t population‑specific. It was systemic—a state that embraced the language of inclusion while maintaining a service system that excluded people in practice.
Hutchinson v. Patrick: When “Community Services” Existed Only on Paper
By the time Hutchinson v. Patrick was filed in 2007, Massachusetts had already been sued repeatedly for failing to provide the services federal law requires. Ricci exposed the state’s neglect inside institutions. Rolland revealed the same neglect in nursing homes. Boulet showed that thousands of people with IDD were left on waitlists with no residential supports at all. Hutchinson continued this pattern — but with a different population and a different kind of abandonment.
Who Were the Plaintiffs?
The plaintiffs in Hutchinson were adults with acquired brain injuries (ABI) who had been warehoused for years in nursing facilities. They were medically stable and entitled under federal law to receive services in the most integrated setting. With the right supports, they could have lived safely in the community. They remained in nursing homes because the Commonwealth had never built the community system the law required.
Nursing facilities are designed for short‑term rehabilitation, end‑of‑life care, medically unstable individuals, and people who cannot be safely supported in the community. The Hutchinson plaintiffs did not fall into those categories. Massachusetts kept them in nursing homes because no community‑based ABI system existed.
Like Rolland, Hutchinson was about people who were eligible for community services but were kept in nursing homes because nothing else existed. All these cases expose the same truth:
Massachusetts has often failed to comply with federal disability law, and substantial reform has only happened with federal court supervision.
And just like Boulet, Rolland, and Ricci, Hutchinson was not a policy disagreement — it was a civil‑rights case. The plaintiffs were not asking for new programs or special treatment. They were enforcing rights that already existed under Medicaid, the ADA, Section 504, and Olmstead.
The state had the obligation. The state failed to meet it. And the court had to intervene.
Two Populations, One Systemic Failure
At first glance, Rolland and Hutchinson seem to involve different populations. Rolland addressed adults with intellectual and developmental disabilities (IDD) who were placed in nursing homes—often without medical justification—and denied the active treatment required under federal law. Hutchinson involved adults with ABI who were kept in nursing facilities for years despite being medically stable and appropriate for community living.
The underlying failure was the same.
Massachusetts maintained a system where federal rights existed on paper but the capacity to deliver those rights did not exist in practice. In Rolland, the state used nursing homes as a default placement for people with IDD instead of developing appropriate community services or maintaining access to intermediate care facilities for individuals with intellectual disabilities (ICF/IID).
In Hutchinson, it failed to create clinically appropriate alternatives to nursing homes for people with ABI.
In both Rolland and Hutchinson, the Commonwealth publicly embraced “community living” while refusing to fund or build the services necessary to make that promise real.
The consequences were predictable. People with IDD remained in nursing homes without active treatment. People with ABI remained in nursing homes without rehabilitation or a path back to the community. Families were told to wait. The state insisted that progress was being made even as thousands of people lived in settings that violated federal law.
What connects these cases is not the diagnosis of the plaintiffs but the state’s recurring behavior.
Massachusetts repeatedly avoided building the services that Medicaid, the ADA, and Olmstead require
—relying on the fact that most families lacked the resources to challenge the system,
and that only federal litigation would force compliance.
Hutchinson demonstrated that the failures revealed in Rolland were not limited to IDD. They reflected a structural problem: a state that spoke the language of inclusion while maintaining a service system that excluded people in practice.
The Lived Experience Behind Hutchinson
For the adults at the center of Hutchinson v. Patrick, the violation was not abstract. It was daily life. These were people who had survived catastrophic brain injuries, completed rehabilitation, stabilized medically, and were ready to return to their communities. Their clinicians agreed. Their families agreed. Their own progress made it clear. Yet they remained in nursing facilities for years—not because they needed to be there, but because Massachusetts had nowhere else for them to go.
Families described a kind of suspended animation. Their sons and daughters were physically safe but emotionally abandoned, living in settings designed for end‑of‑life care rather than recovery. Therapy was minimal or nonexistent. Days were long and empty. Skills gained in rehabilitation slowly eroded. Depression deepened. People who had fought their way back from brain injury were left in places that offered no path forward.
The distance families traveled was measured not in miles, but in the loss of ordinary life. Parents arrived to find their adult children sitting in hallways, parked in wheelchairs, or confined to their rooms because there was nothing else to do. Staff were often kind, but overstretched. Privacy was rare. Autonomy was almost nonexistent.
Life in a Nursing Home as a Younger Adult with ABI
Cathy Hutchinson was in her early forties when a brainstem stroke left her mute and quadriplegic. She collapsed while gardening at her home in Attleboro and was taken first to a hospital, then to a nursing home, where she remained for more than a decade.
The nursing home was designed for older adults, but Cathy was a relatively young woman with decades of life ahead of her. She described the experience in stark terms. Living there, she said, felt like being “in a prison.” She explained further:
“I feel isolated from the real world. I have little to no privacy. I don’t want to live this way, and I can’t think of anyone else who would.” -Cathy Hutchinson
Her words captured what many younger and middle‑aged adults with acquired brain injuries experienced in Massachusetts nursing homes during the Hutchinson years: long-term confinement in settings built for end‑of‑life care, limited privacy, minimal community access, and a profound sense of being cut off from ordinary life.
Cathy became the lead plaintiff in a class action lawsuit arguing that the state was violating the ADA by failing to provide community-based services. After the settlement, she was approved to move into an integrated community residence. When she arrived at her new home in Taunton in 2011, she spelled out a single phrase using her alphabet board: “Thank you.”
What made this especially painful was that everyone knew the truth: these individuals did not belong in nursing homes. They were not medically fragile. They were not declining. They were waiting—waiting for housing that did not exist, for staffing that had never been funded, and for a community system the state had promised but never built.
Across interviews and affidavits, families returned to the same four losses again and again:
- Loss of progress, as hard‑won skills faded without therapy or stimulation
- Loss of identity, as adults were treated as passive patients rather than people rebuilding their lives
- Loss of connection, as distance and institutional routines made family involvement harder each year
- Loss of hope, as months turned into years with no timeline, no plan, and no exit

These were not isolated failures. They were the predictable result of a system that had never built the community infrastructure required by Medicaid, the ADA, or Olmstead. The individuals in Hutchinson were not “hard to serve.” They were easy to serve—if the services the law required had existed.
They were the predictable result of a system that had never built the community infrastructure required by Medicaid, the ADA, or Olmstead. The individuals in Hutchinson were not “hard to serve.” They were easy to serve—if the services the law required had existed.
Their lived experience revealed the same pattern exposed in earlier cases: people entitled to community living were instead confined to settings that stripped them of autonomy, connection, and purpose. The harm was not theoretical. It was lived, every day, for years.
The Settlement and Its Impact
In 2013, the state entered into a sweeping settlement requiring:
- the creation of two new ABI Home and Community‑Based Services (HCBS) waivers
- the development of community residences and supports
- transition of hundreds of individuals out of nursing homes
- improved service planning and oversight
- compliance with Olmstead’s least restrictive setting rules
The case remained under court supervision for years and was not dismissed until 2021.
Once again, Massachusetts expanded services only because a federal court forced it to.
The Real Cost of High‑Acuity Care
The Hutchinson settlement forced Massachusetts to build something it had never built before: a medically intensive community system capable of supporting adults with high‑acuity needs outside of nursing homes. That system required 24/7 licensed nursing, daily therapies, clinical oversight, specialized equipment, and integrated day habilitation—delivered to one or two residents in very small homes. When you replicate nursing‑facility‑level care in tiny settings, the cost rises sharply. That is why the Hutchinson model exceeded $2,000 per person per day.* This cost is federally reimbursable (FMAP reimbursable), so the cost to the state is $1000 per person per day, or $365,000 per year.
This is not an anomaly. It is the actual cost of providing the services that federal law requires for people with complex needs.
Why “Community Is Cheaper” Is a Myth
Massachusetts has long claimed that community services cost less than facility‑based care. But the current Home and Community Based Services (HCBS) system for IDD appears cheaper only because essential services—nursing oversight, therapies, behavioral supports, and habilitation—are often missing. The state has kept costs down by under‑serving people and by shifting the burden to emergency rooms, psychiatric hospitals, and crisis services.
When you compare real, fully funded models, the picture changes. According to the Saving Wrentham and Hogan Alliance cost analysis, ICF/IID services —federally regulated, clinically structured, and staffed for high acuity—cost the Commonwealth $88,939–$260,900 per person annually (after federal FMAP reimbursement, social security payment offsets, and at realistic census levels), with per‑person costs decreasing as census increases. These programs benefit from economies of scale that small community homes cannot achieve.
The lesson is not that community care is unaffordable. The lesson is that Massachusetts has never built the community system federal law requires. When forced to do so in Hutchinson, the true cost became visible. When left to its own devices, the state relies on group homes, day habilitation programs, shared living, extraordinary care provided by parents and siblings, and other solutions that often cannot meet high‑acuity needs and are far cheaper only because they provide far less. They also rely on nursing homes.
Nursing Homes vs. ICF/IID — Both “Institutions,” But Not the Same
Federal law classifies both nursing homes and Intermediate Care Facilities for Individuals with Intellectual Disabilities (ICF/IID) as “institutional” settings. But the similarities end there. The two models were created for entirely different purposes and deliver fundamentally different types of care.
Nursing Homes: Custodial Care, Not Habilitation
Nursing homes are designed for elderly adults and people with short‑term medical needs. Their core function is custodial care—feeding, bathing, medication administration, and basic nursing. They are not required to provide:
- habilitation
- therapies
- behavioral supports
- communication supports
- community integration
- individualized skill development
For people with IDD or ABI, this means stagnation. Residents often spend years without meaningful activities, without therapy, and without any path back to the community.
Intermediate Care Facilities for Individuals with Intellectual Disabilities ICF/IID: A Clinical, Habilitative, Community‑Integrated Model
ICF/IID facilities were created specifically for people with intellectual and developmental disabilities who have medical or behavioral needs. They are federally regulated and must provide:
- 24/7 nursing and clinical oversight
- Active treatment (a legal term requiring continuous skill development)
- PT/OT/speech therapies
- Behavioral supports
- Individualized habilitation plans
- Community integration activities
- Access to employment and day programs
Unlike nursing homes, ICF/IID programs are designed to increase independence, not simply maintain basic functioning.
Community Integration: ICF/IID Often Outperforms Home and Community-Based Services (HCBS)
For individuals with high‑acuity needs, ICF/IID settings frequently provide more community access than HCBS. At Wrentham, for example, residents with significant disabilities participate in:
- supported employment
- community outings
- skill‑building programs
Many of these opportunities are not available in HCBS because:
- staffing is insufficient,
- clinical supports are fragmented,
- transportation is limited,
- and providers lack the capacity to support high‑acuity individuals in the community.
The result is that people who “should” be more integrated in HCBS often end up isolated, while those in ICF/IID settings participate in meaningful community life.
Why This Distinction Matters
When advocates or policymakers treat nursing homes and ICF/IID as interchangeable “institutions,” they erase the very services high‑acuity individuals rely on. The real choice is not “institution vs. community.” It is:
- nursing home (custodial, isolating, inappropriate),
- ICF/IID (clinical, habilitative, community‑integrated),
- or HCBS (appropriate only when the system is fully built and clinically adequate).
For many high‑acuity individuals, ICF/IID is the least restrictive option because it provides the supports necessary to access the community safely and meaningfully.
What Happens to ABI Individuals Entering the System Today
The Hutchinson settlement created a high‑quality, medically intensive community model for a specific group of plaintiffs who had been trapped in nursing facilities for years. But that model did not become the standard of care for all adults with acquired brain injuries (ABI). It existed because a federal court required it, and it applied only to people who were already living in nursing homes. Once the court’s oversight ended, Massachusetts did not build a permanent ABI community system capable of serving new individuals entering the disability and long‑term care system.The state built a model only for the plaintiffs, not for the population.
As a result, adults with ABI who experience a sudden injury today—stroke, anoxia, traumatic brain injury, or other causes—still overwhelmingly enter nursing homes first. If they cannot be safely discharged home, there are few alternatives.
The ABI and Moving Forward Plan (MFP) waivers are designed to help people leave nursing facilities or long‑stay hospitals, not to prevent placement in the first place. To qualify, an individual must already be in a nursing home. And even then, access to community placements depends on whether a provider has capacity, whether a slot is available, and whether the individual meets the waiver’s narrow eligibility criteria.
This means the pipeline that produced the Hutchinson lawsuit remains largely unchanged. ABI individuals who need structured supports, therapies, and clinical oversight are still funneled into nursing facilities because the Commonwealth never built the community infrastructure the settlement demonstrated was possible.
The high‑acuity, court‑mandated services the plaintiffs received were never scaled or extended to new entrants. They were a remedy for a civil‑rights violation—not a system reform. This is the same pattern families of individuals with IDD face today
The result is a two‑tier reality. The Hutchinson class received a court‑mandated, clinically robust community model with 24/7 nursing, daily therapies, behavioral supports, and integrated habilitation. ABI individuals entering the system today receive whatever the existing long‑term care system can offer—which, in most cases, means a nursing home placement, limited rehabilitation, and no guaranteed pathway to community living. The underlying problem that gave rise to Hutchinson persists: Massachusetts still relies on nursing homes as the default placement for people with ABI because it has not built the community system federal law requires.
Hutchinson is not an ABI story—it is a story about what Massachusetts does when confronted with high‑acuity needs.
Why Hutchinson Matters Today
The Hutchinson case is a warning for the IDD community:
- If the state could not build adequate community supports for ABI,
- and could not maintain adequate supports for IDD,
- and could not prevent institutional drift for either group,
…then the current crisis in Day Hab, group homes, and high‑acuity care is not an accident.
It is the predictable result of a system that has never built, or funded the infrastructure required for true community living. Hutchinson shows that the crisis in IDD services is not a new failure—it is the latest chapter in a decades‑long pattern of systemic neglect.
What Comes Next
In our conclusion of our MA IDD Lawsuit Series, we summarize our findings based on our introduction and all four parts of the series.
Previous Installments
To read or listen to the Introduction to our MA IDD Lawsuit series, Introduction: “Why Massachusetts Keeps Getting Sued Over Disability Services,” click here.
To read or listen to Part 1 of our series, “What the Rolland Lawsuit Reveals About Massachusetts’ Real Commitment to Community Living,” click here.
To read or listen to Part 2 of our series, “Ricci v. Okin: The Lawsuit That Forced Massachusetts to Fix Its Institutions,” click here.
To read or listen to Part 3 of our series, “Boulet v. Cellucci: When “Community Living” Meant Waiting Without Services,” click here.
Further Reading on Hutchinson v. Patrick
HOME FREE: Woman moves into Silver City house after escaping nursing home ‘prison’
Taunton Cathy Hutchinson: Lawsuit brings reform for disabled
Join the Saving Wrentham and Hogan Alliance
As we continue our MA IDD Lawsuit Series, we invite families, advocates, and allies to help us document the present crisis and protect the future. Contact Us.
* Massachusetts bills ABI Residential Habilitation under HCPCS T2016 — a per‑diem nursing‑level service — and the state’s own rate filings place that per‑day cost at just over $2,000